Part 1: Introduction to TMSA & Mould Illness/CIRS
Part 2: Tests for Mould Illness/CIRS (Shoemaker Protocol)
Part 3: Tests for Mould Illness/CIRS (Non-Shoemaker, inc. mycotoxins)
Part 4: CIRS treatment protocol (Shoemaker protocol)
Part 5: Building testing
Part 6: Building remediation and mould prevention
Part 7: Conclusion
Mould illness (mold illness, USA spelling) is the common name for CIRS-WDB. The two terms will be used interchangeably throughout this FAQ. CIRS-WDB is a condition caused by biotoxins and inflammagens produced by microorganisms such as mould, bacteria and actinomyces found in water-damaged buildings. Tick-borne infections such as Borrelia (Lyme disease) and Babesia, toxic blue-green algae and ciguatera found in reef fish can also produce biotoxins and cause CIRS.
These conditions are called biotoxin illnesses.
There are three main schools of thought about mould causing health problems.
- The traditional viewpoint is known as the allergy theory. This theory views mould as causing an allergic response that results in upper respiratory symptoms, such as asthma and rhinitis. The typical medical practitioner generally views mould as a minor ailment only. Doctors will usually test for mould allergy via IgE RAST blood tests or skin prick tests. Treatment is centred on exposure reduction and/or immunotherapy. It is possible to have mould allergy and CIRS.
- The second viewpoint is the colonisation/infection theory. This theory views mould as mostly a problem when found growing in the body, either in the gastrointestinal tract (yeast overgrowth), nasal and sinus cavities, skin and/or bloodstream. Stool tests, culture of sinus/nasal cavity or urine mycotoxin testing are usually the way this is diagnosed. This is treated with anti-fungal medications and/or supplements and diet. Binders and other supplements such as glutathione are often used by proponents of this philosophy. Detoxification methods such as far infrared saunas and coffee enemas can be recommended as well.
- The third viewpoint is the Chronic Inflammatory Response theory. This theory views mould and other microbes in water damaged buildings as being able to cause a chronic inflammatory response and a host of symptoms that can persist for years and decades even if removed from exposure, especially in a genetically predisposed subset of the population. This is because those with impaired HLA genetics are not able to mount an effective antibody response to biotoxins and inflammagens found in water-damaged buildings (including, but not limited, to those from mould). As a result, a chaotic and ineffective inflammatory cascade occurs which includes lowering of the regulatory hormones and increase in inflammatory cytokines, dysregulation of gene expression, and atrophy and inflammation in the brain.
Note: One or a combination of the three may be an issue for a patient. TMSA and this document primarily focuses on the CIRS theory.
Dr. Ritchie Shoemaker, MD, from Pocomoke, Maryland, USA is the leading physician and researcher in regards to the CIRS theory. He has published over 20 peer-reviewed papers, on the mechanism, diagnosis and treatment of CIRS. A new organisation, International Society for Environmentally Acquired Illness (ISEAI), formed by several former Shoemaker certified physicians, aims to continue research and education into CIRS, that they term EAI-WDB (Environmentally Acquired Illness due to Water-damaged Buildings), and other environmentally acquired illnesses.
For the colonization theory Dr. Joseph Brewer, Dr. Neil Nathan, Dr. Janette Hope are the leading proponents. See references section for papers.
Why was he reprimanded? Primarily for using several pharmaceutical drugs off-label that were then part of the CIRS/Shoemaker protocol.
– Actos (then used for reducing the intensification reaction)
– Rifampin (then used an an antibiotic for eliminating MARCoNS)
– Procrit (then used for decreasing C4a)
Note: none of these drugs are part of the current protocol.
Remember as CIRS is a relatively new concept and not embraced by mainstream medicine all medications for CIRS are off-label, from cholestyramine and Welchol to vasoactive intestinal polypeptide (VIP). Many Lyme literate doctors have also had reprimands, or worse, due to prescribing of antibiotics and other medications off-label. This is the price of being cutting edge and not accepting current “standard of care” or typical diagnoses for complex chronic illnesses such as CIRS.
Yes. Borrelia species (Lyme disease) and the parasite Babesia (Babesiosis) transmitted through tick bites also produce biotoxins and can cause CIRS even after the infection is eradicated. CIRS can also be caused by eating reef fish contaminated with toxins causing ciguatera, or exposure to bodies of water with toxic blue-green algae or dinoflagellates.
Viruses and, probably, other stealth infections can also contribute to lowered MSH and VIP and may cause, or at least contribute to CIRS. Similarly traumatic brain injury can lower MSH and cause, or contribute to, CIRS. (Shoemaker et al, 2014, [0061])
- Shoemaker, R., & Ryan, J. (2014). US Patent No. 20,140,046,143 A. Washington, DC: U.S. Patent and Trademark Office. Google patents
In a number of ways
- Borrelia and Babseia produce biotoxins that may cause CIRS and account for some cases of Post Treatment Lyme Disease/Chronic Lyme disease; that is the continuing symptoms of Lyme disease/Babesiosis even if the bacteria/parasite has been eradicated.
- Borrelia and Babseia infection can cause an inflammatory cascade that can be the priming event that expresses the genetic (HLA DR/DQ) susceptibility to mould/water-damaged buildings that could be tolerated before (see 2.4 – HLA DR/DQ gene testing)
Reference: Shoemaker, R.C., Giclas, P, Crowder, C, House, D.E., & Glovsky, M. (2008). Complement split products C3a and C4a are early markers of acute Lyme disease in tick bite patients in the United States. International archives of allergy and immunology, 146(3), 255-61. doi: 10.1159/000116362 | PMID 18270493 | Full text
In research Dr. Shoemaker found that 35 health symptoms could be categorised into 13 clusters. If a patient is confirmed to have 8 or more clusters of symptoms the likelihood of presence of CIRS exceeds 95%. A cluster is positive if you have one or more symptoms in each group. When combined with VCS deficits, symptom clusters can yield an accuracy of 98.5%, with false negatives < 2%. (Shoemaker et al, 2017). [Note clusters and VCS cannot differentiate CIRS-WDB from other CIRS causes such as CIRS Lyme].
You can see the CIRS clusters on the symptom page.
- Lyme disease (Borrelia), Babesiosis (Babesia) and other stealth infections (watch this webinar)
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
- Fibromyalgia
- Multiple Chemical Sensitivity (MCS)
- Inflammatory Bowel Disease (IBD), Irritable Bowel Syndrome (IBS), SIBO, Leaky Gut (watch this webinar)
- Alzheimer’s Disease (watch this webinar)
- Mast Cell Activation Syndrome (MCAS) (watch this webinar)
- Multiple Sclerosis (MS)
- Depression
- Post Traumatic Stress Disorder
- Allergies
(cf: common misdiagnoses at Surviving Mold).
The cost is $15 USD although there are discounts for bulk purchasing which are handy if continue with the CIRS protocol.
Dr. Shoemaker’s original research showed a sensitivity of 92.5% with only 7.5% false negative results, although this was done with a handheld device. False positive were even less (2.5%) and mainly seen in those who had been exposed to occupational solvents, heavy metals, hydrocarbons and petrochemicals. In layman’s terms if you are positive via the Surviving Mold test it is very likely you have a biotoxin illness; VCS can also be used to track your treatment.
If you are negative you should go onto other screening and diagnostic testing to confirm or rule CIRS out but you may still be able to rely on VCS to track treatment.
Is there a free one available? (VCSTest.com)
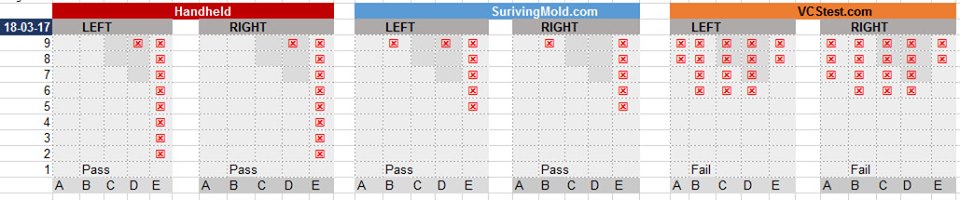
Yes, there is a free test available at VCSTest.com however the results don’t seem to correlate with the handheld or Surviving Mold versions. It’s strongly suggested to do the Surviving Mold test, in addition, if you do the free one first. See the following table for a sequential comparison done by the author in March 2017, comparing the handheld to the Surviving Mold test, to the VCSTest.com one (following instructions given).
2.4.1 What are the HLA genes?
In unpublished research conducted by Dr. Shoemaker of his 10,000 size patient population approximately 25% of the general population have Human Leukocyte Antigen (HLA) genes that are mould, Lyme or multi-susceptible (i.e. susceptible to biotoxins from mould/WDB, and Lyme, and dinoflagellates). When these genes are primed (see 2.4.5 below) and a person is exposed to biotoxins the immune system does not make the appropriate antibodies to clear them due to a defect in antigen presentation. These people will not excrete biotoxins, they instead recirculate in the body for years, if not indefinitely, unless binding compounds are used.
The HLA genes merely indicate genetic susceptibility to biotoxin illness – having them does not automatically mean you have CIRS.
2.4.2 Getting the HLA gene test in Australia
Any GP can request “HLA DR-DQ typing” (NOT “HLA DR/DQ for Coeliac Disease” as previously indicated) but it must be performed at a Sonic Healthcare laboratory for the results to be formatted correctly. See the Resources page (“HLA DR/DQ Gene Test” section) for the Sonic Healthcare division in your state.
It can be if your doctor checks the bulk bill box. The MBS schedule number is 71151.
2.4.3 Interpreting the results
If your doctor is unable to interpret you can put your numbers into the Australian HLA-DR calculator and/or post in the TMSA Facebook group.
2.4.4 Does 23andme show these HLA genes?
No. 23andme does not show all the HLA haplotypes and not in a format that correlates to Dr. Shoemaker’s table.
2.4.5 My friend/partner/child has HLA susceptible genes but they don’t get sick with exposure to water-damaged buildings, how come?
Dr. Shoemaker found that HLA genes generally need to be primed by an inflammatory illness, or event, that causes a cytokine storm such as influenza, Coxsackie virus, Lyme disease, mononucleosis (Epstein Barr Virus/glandular fever) or ECHO virus infections, intense inflammatory lung responses and unusual conditions such as Kawasaki disease. (Berry, 2014, p14)
Following that logic, other events like surgery, accidents, stressful events/trauma and other infections or illness could also be priming events.
However, if there is a great deal of inflammagens and biotoxins in a water-damaged building that can be enough to prime the genes and cause CIRS by itself. (Shoemaker et al, 2006).
References:
- Berry, Y. (2014). A physician’s guide to understanding & treating biotoxin illness. Surviving Mold.
- Shoemaker R, Lipsey R. (2006). Results of health screening and visual contrast testing. St. Bernard’s Parish, Louisiana. Surviving Mold. Full-text
2.4.6 HLA susceptibility in other disease states
This author has put together a Google spreadsheet that summarises many disease susceptibilities, and also disease protection, of the Shoemaker’s HLA haplotypes found in the scientific literature. Autoimmune immune conditions in particular are quite prevalent.
| BIOMARKER | AUS LABORATORY | MEDICARE | FASTING | Normal/Shoemaker Range | NOTES |
|---|---|---|---|---|---|
| TGF-b1 | N/A | 344-2380 pg/mL | NutriPATH is not considered to accurate (see 2.6). | ||
| C4a | N/A | 0-2830 ng/mL | " | ||
| MMP-9 | N/A | 85-332 ng/mL | " | ||
| VEGF | N/A | 31-86 pg/mL | " | ||
| a-MSH | N/A | 35-81pg/mL* | " | ||
| VIP | Local lab -> RPA/SSWP | Y (71151) | Y | 6.8-18.6 pmol/L | SSWPS info page. |
| Leptin | Local lab -> RPA/SSWP | N - Out of pocket cost varies | Y | NR 2-5.6 ng/mL (M), 3.7-11.1 ng/mL (F) | SSWPS Info page |
| ADH (Copectin) | Local lab -> RPA/SSWP | N - Out of pocket cost varies | <7.0 pmol/L | SSWPS info page. Common pattern is low ADH with high osmolality | |
| Serum Osmolality | Local lab | Y | 280-300 mmol/kg | Interpret with ADH | |
| HLA DR/DQ | Sonic Group or NutriPATH | Y (66695) | Sonic page | ||
| ACTH | Local lab | Y | Interpret with cortisol | ||
| Cortisol (AM) | Local lab | Y | Pattern can be low ACTH and low cortisol but sometimes high ACTH, high cortisol. | ||
| Anti-gliadin antibodies | Local lab | Y | 0-19 (IgA, IgM) | Sometimes elevated in CIRS. | |
| Anti-phospholipid antibodies | Local lab | Y | 0-12 (IgA), 0-10 (IgG), 0-9 (IgM) | Sometimes elevated in CIRS. | |
| DHEA | Local lab | Y | Often low | ||
| Testosterone (total & free) | Local lab | Y | Often low | ||
| Estradiol | Local lab | Y | Often high |
NutriPATH’s biotoxin/mould blood tests and panels (apart from HLA DR/DQ and MARCoNS) cannot be recommended at this time due to inaccuracies compared to Quest Diagnostics.
Reference: Mold Illness in Children webinar (35m) and Low Tox Life podcast episode 55.
No other Australian diagnostic testing for TGF-b1, VEGF, C3a, C4a, MMP-9, MSH currently available. Dr. Gupta is looking at sending to LabCorp in 2020.
It is still an experimental test at present and therefore should not be used for diagnosis. However, it can be a tool to track inflammatory and atrophy changes at baseline and throughout treatment. Dr. Ackerley believes the Triage Brain Atrophy Report (TBAR), that takes into account normal ranges for patient sex and age, is more accurate than the general morphology report alone, and the spreadsheet that was previously used.
Multiple Antibiotic Resistant Coagulase Negative Staphylococci (MARCoNS) are bacteria that colonise the nasopharynx area forming biofilms and creating exotoxins. These form due to low levels of MSH in mucous membranes which is antimicrobial and antiinflammatory. MARCoNS can themselves further lower MSH. Dr. Shoemaker sees MARCoNS colonisation in 80% of CIRS patients. See the Biotoxin pathway diagram to see how hormones and immunity are affected in CIRS.
- Obtaining the collection tube
- Direct from Microbiology Dx
Order swab kit from Microbiology Dx free of charge. Go to the ‘Order Collection Kits’ page and fill in the details. You’ll need to put Australia onto the ‘City, State, Zip’ field. You will need to include your doctor’s details on the web form. Ideally email them and ask for the Remel® BactiSwab™ wire shaft transport swab – although the default swab will suffice.
Alternatively you can use an aerobic nasal swab from your doctor and get your doctor to fill out the requisition form. - NutriPATH
Order a kit via NutriPATH, who send it on to Microbiology Dx.
- Direct from Microbiology Dx
- Performing the swab
- This can be done by a doctor or patient. The swab needs to go through the nose right up to the back of the throat, about 3 inches. Swivel the swab for 3-5 seconds when you reach the throat. It is unpleasant but not painful. Read the Microbiology Dx instructions or read the blog post on Biotoxin Journey for directions.
- Sending swab to Microbiology Dx
- When used with the correct swab, the sample is viable for up to 30 days. There are several options for sending it to Microbiology Dx. Write “non-infectious sample” on the customs form.
- Australia Post air mail letter ($2.75). The cheapest option.
- Australia Post’s EMS Courier (approx $57-58).
- FedEx. Supplied with the kit from Microbiology Dx (approx $80).
- When used with the correct swab, the sample is viable for up to 30 days. There are several options for sending it to Microbiology Dx. Write “non-infectious sample” on the customs form.
- Sending swab to NutriPATH
- Follow the instructions in the NutriPATH kit.
- Cost
- Currently the cost for MARCoNS and other bacteria with sensitivities is $85 USD. The results will be emailed to your doctor. NutriPATH is more expensive ($150 AUD).
- Fungal culture testing
- Dr. Shoemaker strongly disagrees with treating fungal colonies (see 4.3.3 – Nasal fungal colonisation and anti-fungals, below) while some other doctors do. This is an additional cost ($80 USD) and takes longer to report than MARCoNS.
- Biofilm testing
- This is optional ($100 USD) but can be useful as it tells you if any biofilm is present and at what strength. Dr. Shoemaker originally deduced that MARCoNS produced biofilm when they were resistant to 2 or more antibiotic classes but this may not always be the case.
- Interpretation
- If the culture reveals coagulase negative staph which are resistant to two or more antibiotics then you are positive for MARCoNS and should be treated with a suitable nasal spray (see 4.3.2 MARCoNS Treatment). The amount (“large amount” etc.) is not important. If the culture is methicillin resistant you may herx more when using anti-microbials. Staph coag positive (golden staph), staph coag neg with only one antibiotic resistance, non-staph bacteria, as well as fungus (if requested) are common findings and do not need to be treated generally.
Two laboratories, Realtime (available via NutriPATH) and Great Plains (available via RN Labs) currently offer urine mycotoxin testing in Australia.
There is a great deal of debate among health professionals about the utility of urinary mycotoxin testing. Doctors such as Neil Nathan and Jill Carnahan find them helpful.
Dr. Shoemaker does not recommend these tests for a number of reasons:
- Mycotoxins make up < 10% of the burden of inflammagens in a WDB.
- These tests only look for one to two dozen mycotoxins when there have been four hundred discovered so far.
- These tests are polyclonal and have never had specificity of their antibodies confirmed (Realtime test).
- Urine mycotoxins are generally confounded by mycotoxin ingestion from common foods such as grains, corn, peanuts, tree nuts, chocolate and coffee.
See Dr. Shoemaker 2015’s Hopkinton Lecture (2:24:53. Thoughts on Realtime Labs) and Dr. Joseph Brewer: Nasal fungi, anti-fungals and junk science.
His company MyMycolab provides testing of IgG and IgE antibodies of 12 different types of mycotoxins in blood serum. He believes the IgE response occurs when there is a large exposure to that particular mycotoxin, and has mast cell invovlment, while IgG responses are indicative of lesser amounts of exposure. Unlike antibodies to mould spores mycotoxin antibodies are short lived and should reduce after 6 months of avoiding exposure.
Testing ($380 USD) can be ordered and drawn by those in Australia and shipped back via FedEx.
Mould allergy testing tests for an IgE allergic reaction to certain species of mould spores, usually a mould mix, and not mycotoxins. This is usually done via skin prick testing or blood RAST testing. This is a common test offered by most laboratories, covered by Medicare, and often the only mould-related test most GPs or allergists will know of and worth doing.
As stated previously mould allergy is an adaptive immune system antibody response and is different from CIRS which is a chronic innate immune system response. It is possible, but not that common, to have both mould allergy and CIRS.
ArminLabs in Germany, known for their Borrelia and co-infection testing also offer EliSpot testing for Aspergillus Peptide Mix 1 & 2. This tests for the cell-mediated, rather than the humoral (antibody), arm of the adaptive immune system.
The Shoemaker protocol is a systematic treatment plan consisting of several steps that need to be followed in order. The full protocol consists of 11 steps, however depending on biomarkers and symptoms not all steps may have to be followed. Only the main steps are outlined here.
This is of paramount importance but is often the most difficult step. One must live, work and otherwise spend time in/visit buildings with a HERTSMI of < 11 at a minimum. Otherwise you’ll continue to be exposed to inflammation causing biotoxins and inflammgens. If re-exposed to another water-damaged building you may need to re-start the protocol from this step.
The most well-known mould avoider is Erik Johnson, who was the prototype for CFS in Lake Tahoe, Nevada in the mid-1980s. He was effectively symptom free with extreme mould avoidance only, and did not follow the rest of the Shoemaker protocol. For more on Erik’s story and mould avoidance techniques read the book Back from the edge by Lisa Petrison (see resources).
Ideally the use of binding medication is done once clear of water-damaged buildings, although binders can be initiated if still exposed.
Dr. Shoemaker’s preferred binder – Cholestyramine (CSM)
Cholestyramine (CSM) is a sixty year old cholesterol lowering medication which has been extensively studied and has an excellent safety profile. This negatively charged binding resin attracts positively charged biotoxins from bile and excretes them in the feces. It is not absorbed systemically. It is available in Australia either as Questran Lite, which contains aspartame or as a pure compounded version. The compounded version may contain stevia and various forms of cellulose, which are harmless excipients in the vast majority of people. See resources for compounding pharmacies. The full dosage is four grams four times per day (QID), thirty minutes before meals/medications or one hour after meals/medications. It is suggested you start with a small dose (1-4 grams) and work your way up to the full dose.
Are there any side-effects?
CSM can have some gastrointestinal (GI) side-effects such as constipation, gas and acid reflux. Constipation can usually be ameliorated with magnesium citrate/ vitamin C/ soluble fibre (chia seeds, flax seeds and psyllium). Long term use can deplete fat soluble vitamins (A, E, D, K, Co Q10) so it is suggested to supplement those, away from CSM dosing. It is also advised to increase healthy fats in the diet such as eggs, butter/ghee, coconut oil, avocados and olive oil.
Dr. Shoemaker’s second binder of choice – Welchol
Welchol (colesevelam) is a medication similar to CSM. It generally causes less GI side effects, and can be taken with food. It is the binder recommended by Dr. Shoemaker for sensitive patients who can’t tolerate CSM. One caveat is that it only has 25% of the binding capacity of CSM. Also it can only be obtained at a select number of compounding pharmacies in Australia. Dosage is two tablets (625mg) two to three times per day.
How long do I stay on binders?
A minimum of one month with the average time being six-twelve months, although some people stay on it for longer. Duration is dependent on the VCS being passed, symptom reduction and absence of exposure to further water-damaged buildings. Some people stay on a lower maintenance dose (4 grams, twice a day) on a continual basis or prophylactically, taking it short term when re-exposed to WDBs (full dose, 3-7 days after exposure).
Non-systemic binders (these stay in the GI tract)
- Activated charcoal – A broad spectrum binder, that has been used in animal mycotoxin and endotoxin (bacterial toxin) studies. Can also bind pesticides and VOCs. May bind with nutrients, so, as with CSM it is best taken away from supplements and medications. Suggested dose: 500-1000mg, 2-4 times per day. Suggested brands: Bulletproof, Blants (powder form) and Nature’s Way. Caveat: it will cause darkening of stools.
- Chitosan – Similar in structure to CSM and Welchol and has a similar lowering of cholesterol of those medications but may also have anti-microbial and anti-cancer properties. Caveat: Derived from shellfish. (1, 2, 3). Suggested dose: 500-1000mg, 2-4 times per day. Suggested brands: Now, Nutricology, and Natural Balance.
- Bentonite clay (aka montmorilonite). Binds to mycotoxins (1, 2), bacterial toxins (1, 3), pesticides (1), and heavy metals (1). Suggested dose: 1-3 grams, 2-4 times per day. Suggested brands: Blants, also widely found on eBay (make sure it is marked for human consumption/internal use).
- Zeolite clay (aka clinoptilolite) – Similar to bentonite clay. Established as a mycotoxin binder in animal studies (1, 2, 3). Suggested dose: as per bentonite. Suggested brands: Vita Pure (LavaeVitae), Zeolith MED, Toxaprevent, ZeoBind (BioPure)
- Chlorella – TBA
Note: Dr. Shoemaker didn’t find that any of these were of benefit statistically speaking but your results may vary and some may be helpful adjunctive therapies.
Systemic (these are absorbed into the blood stream)
- Nanoised zeolite – e.g. TRS, ACT. These are zeolite that are small enough to be absorbed into the blood stream and cells from the gut. As with normal zeolite mainly thought of as a heavy metal chelator. (No peer reviewed studies found for nanoised zeolite and chelation or binding, refer to zeolite research above).
- Modified citrus pectin – A fibre from citrus peel that is known to bind to heavy metals, especially lead, and environmental toxins. Also has anti-cancer/anti-galectin 3 effects. Brands include Pectasol-C, Now. (1, 2, 3, 4).
- Glutathione – The body’s master antioxidant. Can also add in detoxification of toxins, including mycotoxins, and heavy metals. Can be in various forms including liposomal, intravenous, intranasal, N-acetyl-cysteine (a precursor) and L-glutathione.
Binders specific for heavy metals
- EDTA, DMSA, DMPS – Tried and tested compounds used in heavy metal chelation.
- Silica – Mainly known to bind to metals especially aluminium, but also thallium and tin. Brands include Biosil and Jarrosil.
- Thiol-functionalized silica – Quicksilver Scientific have a proprietary product, Intestinal Metals Detox (IMD) that is purported to bind to many heavy metals. (1).
Combination formulas
- Ultra Binder (Quicksilver) – Bentonite clay, activated charcoal, chitosan, aloe vera, IMD, arabic gum. Available from ProHealth.
References
- Shade et al. (2018). A Push-Catch System That Enables Effective Detoxification. The townsend letter, February/march 2018. Link.
- Huwig, A., Freimund, S., Käppeli, O., & Dutler, H. (2001). Mycotoxin detoxication of animal feed by different adsorbents. Toxicol Lett, 122(2):179-88. PMID 11439224
- Wilson, T. (2017). Are you detoxing with the correct binders. Sophia Health Institute. Link.
CSM and nasal sprays can cause intensification reactions commonly but incorrectly referred to as herxing, or a herx, especially in Lyme patients. This is because as biotoxins enter the bloodstream, instead of cell receptors, they cause a rise in inflammatory cytokines.
Symptoms will generally exacerbate along with worsening of VCS, in columns D and E, and MMP-9 will increase.
Start these interventions from 30 to 10 days before you start CSM. If intensification gets too much either lower the CSM dose or stop and then follow the intervention(s) below for 5-10 days before restarting CSM.
- No amylose diet
- A no amylose diet enhances the effectiveness of Actos or fish oil by a factor of 500.
Amylose is found in most grains, vegetables grown below the ground (root vegetables) and bananas. Read Dr. Shoemaker’s book Lose the weight you hate for in-depth advice. Similar diets include low carbohydrate, grain free, paleo diets such as the Bulletproof diet, Wahls Diet or Doug Kaufman’s Phase I diet for at least the duration of CSM treatment.
- A no amylose diet enhances the effectiveness of Actos or fish oil by a factor of 500.
- High dose fish oil
- High dose fish oil can lower inflammatory cytokines and other inflammatory markers. Dr. Shoemaker suggests a dose of fish oil where the daily total of EPA at least 2.4 grams per day and DHA is 1.8 grams for 10 days, with CSM started on day 6. Many people stay on this high dose fish oil for longer.
Overweight patients with leptin levels above 8 may have more success with Actos (pioglitazone) a medication for diabetics at 45mg for 10 days (CSM started on day 6) although this is being used less by CIRS doctors due to its black box warning.
- Current Recommended Treatment – EDTA plus colloidal silver nasal spray
- If positive for MARCoNS the usual treatment is at least 30 days, but in reality it can take months, of EDTA/colloidal silver nasal. EDTA helps break down the biofilm and the colloidal silver is an effective antimicrobial with some anti-biofilm activity as well.
- Past Treatments
- Previously BEG nasal spray was used which contained Bactroban, EDTA and Gentamicin. With the increase of antibiotic resistant MARCoNS strains, and studies done by Dr. Joseph Musto of Microbiology DX showing the effectiveness of colloidal silver, the protocol has been changed.
- Alternative treatments
- Neti pot or nasal spray of water with iodine or salt or xylitol (e.g. xyclear).
- Colloidal silver nasal spray by itself may help.
- Nebulised PVP-iodine is very effective according to Greg Muske of Biotoxin Journey. Read his detailed MARCoNS, More MARCoNS and Even more MARCoNS blog posts for more details.
- Follow up testing
- After one to several months of treatment it is recommended to repeat the MARCoNS test. If still positive, consult with your health practitioner for treatment options.
Dr. Shoemaker vehemently discourages the use of nasal anti-fungals. For two main reasons:
- The rates of fungal colonisation in the nasal passages in CIRS patients is the same as healthy controls
- Anti-fungal use can cause anti-biotic resistance to nasal bacteria such as MARCoNS as fungus and bacteria can transfer genes to one another.
See Dr. Joseph Brewer: Nasal fungi, anti-fungals and junk science.
Some other doctors such as Dr. Brewer and Dr. Neil Nathan have been advocating, and publishing studies, on the use of nasal anti-fungals in ME/CFS.
Dr. Shoemaker advocates a gluten free diet, especially if positive for anti-gliadin antibodies. Other steps to balance hormones and reduce inflammatory markers may be required and treated for, please consult with your health care practitioner.
Vasoactive Intestinal Polypeptide (VIP) is a neuropeptide hormone that is predominately made in the hypothalamus and along with MSH is critical in controlling inflammation and the immune system. In a 2013 study, and in clinical practice, Dr. Shoemaker found that VIP:
- Increased plasma VIP levels
- Reduced symptoms to the level of healthy controls
- Reduced inflammatory cytokines (TGF-b1, C4a, MMP-9)
- Increased VEGF
- Balanced Treg immunity
- Increased 25-Vitamin D levels
- Normalised low testosterone levels in Males
- Normalised high estradiol (estrogen) levels in Males
- Increased tolerance to water-damaged buildings
However the caveat to VIP therapy is that if you’re still being exposed to biotoxins from water damaged buildings or MARCoNS then instead of reducing inflammation VIP can increase it (TGF-b1, C4a). It is therefore imperative then that the following conditions must be met before using VIP spray.
- You live, work, study in buildings with a HERTSMI-2 score of < 11
- You pass the VCS test
- You test negative for MARCoNS
- You have normal lipase levels
My VIP level is normal, can I still benefit from VIP spray?
Yes. VIP has wide ranging effects apart from repleting VIP plasma levels. If you still have symptoms even with a normal VIP level, VIP may help.
While your sense of sight, smell and touch are useful tools for identifying mould and feeling dampness much of the time mould and bacterial overgrowth is not visible or odorous.
- Professional inspection by an Indoor Environmental Professional (IEP), mycologist or building biologist with ERMI/HERTSMI-2 testing.
- Professional inspection by an Indoor Environmental Professional (IEP), mycologist or building biologist without ERMI/HERTSMI-2 testing.
- Self inspection and testing via ERMI/HERTSMI-2
Dr. Shoemaker endorses ERMI/HERTSMI-2 by IEP or patient for determining mould levels in a building. The HERTSMI-2 can be derived from the ERMI test.
ERMI stands for Environmental Relative Moldiness Index and was developed in conjunction with the EPA to determine the mould burden of a building using quantified PCR (DNA) testing of settled dust. The ERMI is able to detect full spores and spore fragments which can be 500 times more numerous than intact spores and which most of the biotoxins and inflammagens are attached to.
ERMI is a QPCR mould test and a score calculated from the test. ERMI tests for 36 species of indoor (21) and outdoor mould (14). The ERMI score is derived from subtracting the latter from the former.
HERTSMI-2 is a score, that focuses on five of the most toxigenic mould species, derived from the ERMI. However you can get a stand alone HERTSMI test which only tests for those 5 species.
It is generally recommended to do an ERMI first as it provides you with much more information and calculate the HERTSMI from that. If repeat tests are required, after remediation, or if you are screening properties to rent, then just a HERTSMI may suffice.
- HERTSMI-2 Total > 15: This building is permanently off-limits to those with CIRS.
- HERTSMI-2 Total 11 – 15: This building must be remediated before those with CIRS can enter.
- If HERTSMI-2 Points < 11: This building is most likely safe for CIRS people.
Use the HERTSMI calculator to determine the HERSTMI from the ERMI report.
Note: Some particularly sensitive people may need a lower HERTSMI than 10.
The ERMI score has been depreciated as Dr. Shoemaker and mycologist David Lark determined HERTSMI-2 is more accurate than ERMI to determine if CIRS patients will relapse in a building. Previously, however, an ERMI score of 2 or below was considered safe for those with CIRS for re-entry. However if your MSH is less than 35 and your C4a is higher than 20,000 then the safe level reduced to -1 or below.
MouldLab is currently the only company doing ERMI testing in Australia. MouldLab will give you a kit with either a vacuum attachment or a Swiffer cloth (similar to a pledge cloth). Most people use the Swiffer cloth method. If using the Swiffer method you will wipe down dusty surfaces in one direction, don’t wipe back and forth, in the room(s) you want to test. Generally these are the master bedroom and living room. You should aim to have both sides of the cloth covered with approximately 80% of visible dust. Good surfaces to dust are the topside of ceiling fans, desktop fans, light fittings, top of cupboards, bookshelves, fridges, painting and poster frames, underneath the fridge, fridge coils and underneath furniture.
Avoid window and door areas and floor or skirting boards and do not dust visible mould as this may skew the results. Use latex/plastic cloves when performing dusting so no cross contamination occurs. Put the cloth in a plastic zip lock bag and mail to MouldLab with the completed forms.
Mould remediation is the technique of stopping moisture intrusion to a building, removing water-damaged building materials and removing mould spores, mould fragments, bacteria and biotoxins so a building is safe enough for those with CIRS to enter without relapsing.
This is primarily going to have benefit when your ERMI report shows moderate water saturation moulds such as Aspergillis penicilloides, Aspergillis versicolor and Wallemia sebi. If there is an excess of other species, particularly Stachybotrys and Chaematomium which indicate higher water saturation and possible ongoing water ingress in the house, the services of a professional remediator may be needed. In uncertain cases it is recommended to consult experts such as mycologists, indoor environmental professionals or building biologists on the best way to proceed with remediating a property.
Basement/Garage – Basements are notorious for damp. Look for rising damp. Some have a dehumidifier on 24/7 in these areas.
Roof – Flat roof buildings will develop water leaks sooner or later, avoid. Look for leaks in all roofs, especially in old roofs and cement tile roofs which can be porous in little as 9 years (David Lark). USB data loggers can be used to detect high humidity levels in crawlspaces under roofs.
Attic/crawlspaces – Check for leaks coming from the roof and walls. Also for humidity and condensation in these areas.
Airflow – Draughty buildings are often mould free. Consider ceiling fans and desktop fans, good exhaust fans in bathroom and kitchen and opening of windows as much as possible.
Air conditioners – Due to condensation can be mould havens. Check inside also piping.
Kitchen – Around and under sink for water leaks and water splashing. Sinks are often not properly attached to bench allowing leaks to the particleboard below. Piping can develop pin hole leaks, especially plastic piping, in less than a decade from new. Check dishwasher inside (use vinegar in a wash) and pipes for leaks.
Bathroom – Dehumidifiers and fans are useful tools here. Squidgy showers after use. Mould growth in grouting is a common problem. Aim for good ventilation.
Bedroom – Try to make clutter free with nothing under the bed, that is slatted, to help airflow. Open wardrobe doors for airflow.
Furniture – Non-porous (leather, vinyl) can usually be cleaned and HEPA vacuumed. Porous furniture usually needs to be trashed after water damage.
Books/paper/photos – Photos can be cleaned. Scan and throw away books and paper documents or put in storage.
Carpets – These act as reservoirs for mould, bacteria and dust mites. If water damaged they generally need to be thrown out. If cleaned use a fast drying steam cleaning (e.g. Chemdry).
Clothes – Can be washed with normal washing powder and then dried in sun. Some people have used borax and/or vinegar or clove oil.
Bedding – Mattresses, pillows and quilts are notorious for mould, bacteria and dust mites. Use a whole mattress protector around mattresses. Wash and air in sun blankets, sheets and quilts.
Fridges/washing machines – Notorious for low-level leaks. Should be moved and the underside and back areas thoroughly inspected. In one particularly bad case of water damage in Australia, the culprit was a water pipe to a fridge which had been gnawed by a rodent of some kind.
Dr. Shoemaker is currently testing a specific brand of photocatalytic air purifier while monitoring inflammatory blood markers in a patient cohort.
You must be logged in to post a comment.